FOLLOW US
FOLLOW US





Using the most appropriate setting of care is one of the best ways to reduce health care costs. One way the ACG System supports this approach is within its unique methodology to classify Emergency Department (ED) visits, so users can identify groups of patients who went to the ED but could have been treated at a lower level of care, such as an Urgent Care or Primary Care Provider (PCP).
ACG System expert user Vital Incite, a population health consulting company that helps employers reduce health care costs and increase employee health, recently utilized the ACG System’s ED classification system to reveal a huge opportunity for cost savings with their customers. Using insights from the ACG System, Vital Incite was able to develop a comprehensive action plan for one employer to reduce avoidable ED utilization.
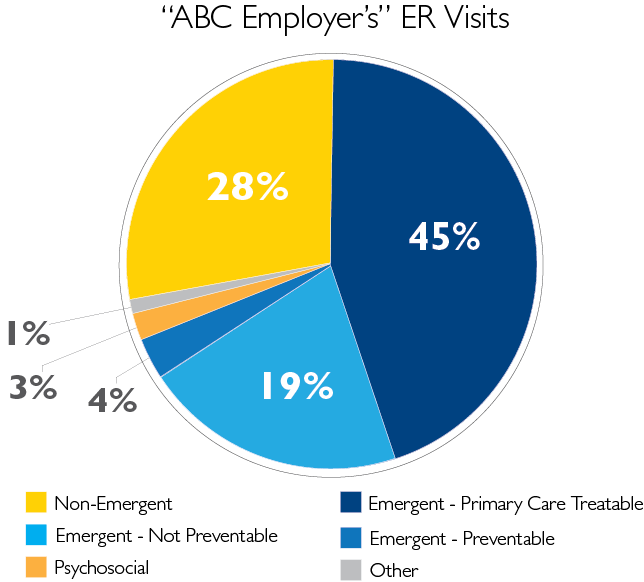
Vital Incite’s analysis began with a review of overall trends. Among Vital Incite customers, similar to national findings, an average ED visit costs approximately $4,300, whereas a PCP office visit averages to about $170. To understand the magnitude of opportunity, Vital Incite first pulled overall ED categorization from the ACG System. In the case of one specific customer, who we will call “ABC Employer,” 28% of ED visits within a 12-month period were for non-emergent diagnoses, and a further 45% were treatable in primary care – resulting in more than two thirds of ED visits being unnecessary.
Vital Incite’s analytics team drilled further to understand day-of-the-week trends among avoidable visits, as well as visit patterns among those patients with and without a strong PCP relationship. The ACG System can identify patients who have no evidence of seeing a PCP or generalist on an ambulatory basis, but who have multiple ED visits for conditions that are non-emergent or primary care treatable, based on the Johns Hopkins ED visit classification.
For “ABC Employer,” there were a total of 611 non-emergent ED visits, with the highest number of visits occurring on Fridays and Saturdays. The analysis of the visits also showed that the majority of the visits were made by their employees, who already had access to an onsite clinic at their workplace.
Among employees with no attributed PCP provider, 30% of ED visits were non-emergent and 44% could have been treated in primary care – representing an enormous opportunity to improve these employees’ PCP use or direct them to onsite clinic resources.
Vital Incite used these findings to recommend a comprehensive strategy to “ABC Employer” to improve PCP use and reduce ED utilization. These specific and targeted strategies to reduce the number of unnecessary ED visits in the next year include:
Ultimately, the ACG System’s ED classification system revealed not only a massive opportunity for cost savings, but also a clear path forward for how to accomplish it.
For more information on this ED classification project, visit Vital Incite’s website or download their detailed case study.
To read more articles from the ACG System on this topic, click here.
Follow Us

